PIOA Supervision Trip in Popondetta, Papua New Guinea (PNG) November 2017
Dr. med. Philipp F. Stillhard, General- and Trauma Surgeon, incl. Orthopaedic Trauma
Popondetta
Popondetta is the capitol of Oro (Northern) Province in PNG and is not far from the beginning of the Kokoda Trail, made famous during World War II. Popondetta Hospital is responsible for over 300.000 people in this area. The town is small, some shops and one hotel, which has a simple infrastructure but it has everything what you need up here and it is special secured by a high fence around the property and a security guard is doing his rounds at night.
PIOA trainee Dr. Alois Mouemuem is working in a small team with a fellow resident, Jimmy, and a consultant, Dr. Opom. The buildings are several decades old but well maintained. The surgical ward accommodates general surgical patients and orthopaedic trauma patients. Energy and water supply seems more or less sufficient. Right now, 2 ORs are running with a small sterilisation and packing unit. Clinical nurses provide an anaesthetic service which is working quite well and efficient. Basic instruments and reposition clamps are available as well as a hand-drill. Recent orders, such as a small and large fragment set is available as well. Basic procedures such as external fixations, pin tractions and uncomplicated small- and large-fragment cases can be done safely. For more complex cases or just for simple K-wire usage, a power drill should be purchased, better with a quick coupling than a Jacobs chuck. Unfortunately, there is no intraoperative imaging available right now.
The OR team is working very thoroughly and clean. Some ideas how the material and especially the different reposition clamps should be packed and stored should be discussed as well as a screw rack would be helpful to get a screw overview during the operation.

An amazing new building in high quality standard is built on the hospital’s property, including 2 new ORs with a C-arm and a casting room with its own x-ray machine, a sterilisation and packing room and a huge recovery room, including 2 ventilation places for patients who need some artificial respiration. Hopefully, it will be opened soon early next year 2018.
During my stay in Popondetta, my main aim was to supervise Alois, as a PIOA trainee and to evaluate the hospital for future supervising visits because working together with the trainees in their environment and with their equipment and possibilities will be an important mean of teaching and transferring knowledge in the future (Walliser M.: SST Mission PIOA Module Apia, Samoa and Kokopo / Kavieng, Papua New Guinea June-July 2017).
A warm welcome was organized at my first day with everybody important from the hospital, followed by lunch. We have been recruited patients from the surgical ward and from the out-patient clinic. Just some cases to mention:
Case 1: Around 60 years old lady with a delayed-union at the right proximal humerus. Because of pain and dysfunctional movements, the right upper extremity is useless. The aim of this case was that this old lady can use her arm again. From the side of teaching aspect, there are three main goals. First, it is important to know the difference between delayed-union and non-union because the treatment is or could be different. Secondly, there is the issue of the different possible approaches around the humerus. After discussing the benefits and drawbacks, we have decided to go for an anterolateral approach which was never done before by Alois. Finally, there are the AO-principles, which should be respected when we go for an operative treatment. In this case, we reached the stability by drilling eccentric during using a large fragment DCP.

Case 2: Old lady, hit by a grass-knife at the right elbow. The x-ray showed an olecranon fracture. We discussed the different treatment possibilities and came up that tension band wiring, especially this technique is unknown in Popondetta, is a great and cheap option for fixing olecranon fractures.
Case 3: However, there are a lot of dislocated forearm fractures in this area. Most of them reach the hospital after some weeks, already nearly healed in a mal-position. This case shows a 4 weeks old right distal radius shaft fracture. The patient can’t hardly do any pronation or supination.

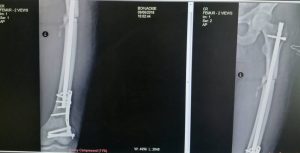
Next to these cases, we did a lateral approach for a distal femur fracture, some tendon repairs and a lot of children fractures for open and closed reductions.
But not only operating was a main issue. We had some good discussions with the hole group about x-rays, reposition techniques, non-operative versus operative fracture treatment, different approaches to the femur, radius and humerus, principles of osteosynthesis, and influence of the patient factors and the injury.
And of course, free-time was also there. I learnt from the “hospital gang” how to play dart and billiards and they showed me places around Popondetta.
I am grateful for this effort.
Future ideas
For sure, more supervision missions should be organised for the Popondetta Hospital. There will be new options with the opening of the new theatre in 2018 meaning that better conditions such as a C-arm could be used for procedures. Furthermore, Sign-Nails should be organised and introduced to the guys up here. Dr. Alois is motivated, has the power, cleverness and knowledge, that he could deal with the Sign-Nails after some supervision.
The hospital should keep going on with buying some implants and screws. To mention only one deficiency, shorter sizes of screws in the large fragment set already run out. In my opinion, a power drill should be purchased, better with a quick coupling than a Jacobs chuck.
Another issue to mention is, that there is a need of teaching the OR-nurses how to use orthopaedic instruments and how they should maintain these instruments because these instruments are quite a new topic in the hospital and of course dealing with it is not easy and has to be learnt.
I am pretty sure, also the anaesthetic team would profit from some supervisor visits and beginning in time in the morning is one important thing next to the different techniques in anaesthesia.
Philipp F. Stillhard, Kavieng 03/12/2017









 This was the first time a power-drill was used up here and I did some training with Thomas and his team including the OT-team how to prepare and sterilize.
This was the first time a power-drill was used up here and I did some training with Thomas and his team including the OT-team how to prepare and sterilize.
