Report PIOA Visitation in Lae, Angau Memorial General Hospital
05.06.2018 – 15.06.2018
Dr. med. M. Walliser, Dr. med. Philipp Stillhard
Aims and outlines of the project:
Two program participants of the PIOA trauma program in PNG have been selected for a supervisory visit. Both participants are acting as HOD of the trauma departments in their hospitals, in this way ensuring a certain continuity in leadership and position. Both of them are qualified and experienced surgeons with good communication skills and reliability.
Dr. Steven James, head of the surgical department of AMGH and participant of the PIOA program since the Madang module in February 2018, was selected for the first time. The SIGN nail should be introduced and instructed in this hospital.
Dr. Kevin Lapu, also HOD of surgery in Nunga Hospital, Rabaul, has already been visited in April 2018 (Dr. med. Philipp Stillhard), this visit was planned as continued training especially in the field of plate osteosynthesis and external fixators.

Angau Memorial General Hospital (AMGH) in Lae, 05.-15.06.2018:
Dr. Steven James is a general surgeon, undergoing orthopaedic / traumatologic specialization. Two additional consultants, 4 registrars and 4 residents are completing the team. The orthopaedic ward has a capacity of 80 beds. There are 4 operating theatres, three actually in use. Instruments and implants for trauma surgery are available (good array of basic instruments, reduction clamps, small and large fragment sets, K-wires, external fixator, air-drive, C-arm and most recently a SIGN set for intramedullary nailing).
Daily ward rounds and clinics (bed-side teaching, case discussions, OP planning) and operations were parts of the daily routine.
Main surgical activities:
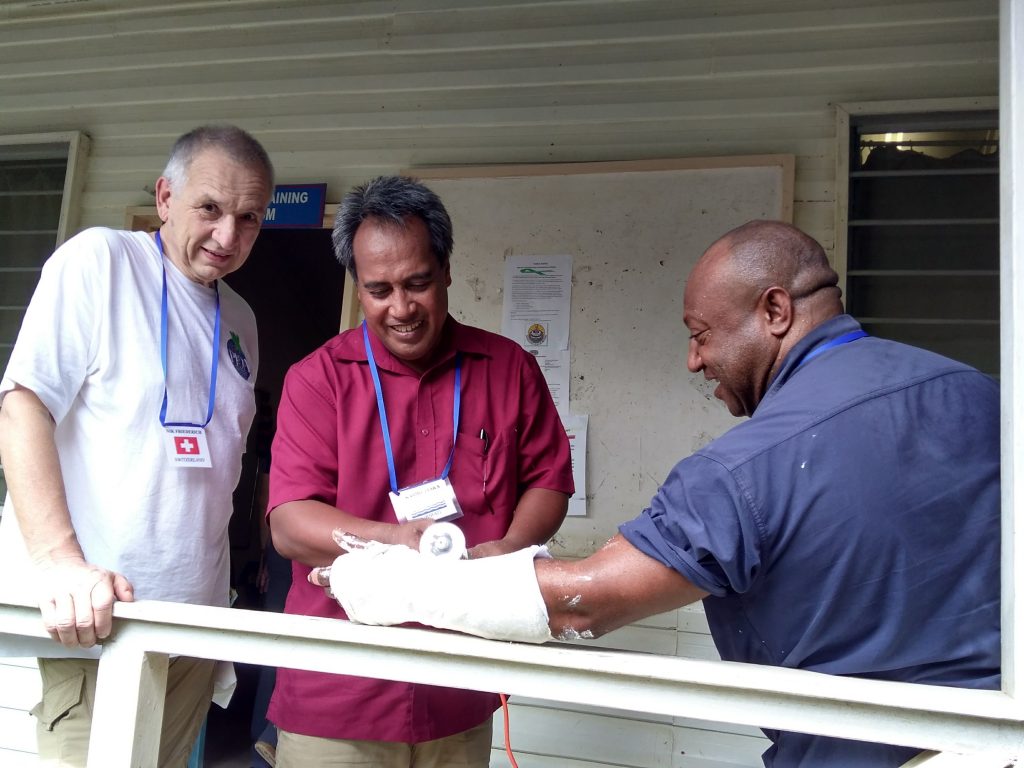
As common in PNG, most patients are presenting late after open fractures (the most common reason for admissions to the trauma ward), resulting in soft tissue and bone infections as well as soft tissue defects. Debridement, soft tissue management and temporary fixation is the most important surgical procedure in order to prepare definitive fixation.

 The introduction of the SIGN intramedullary nailing system was the most important goal of this mission. We were able to operate on several tibial and femoral fractures.
The introduction of the SIGN intramedullary nailing system was the most important goal of this mission. We were able to operate on several tibial and femoral fractures.
The standard approach in displaced simple fractures: Open reduction, standard antegrade nailing and distal interlocking with the aiming device. During the first independent phase, Steven will start with simple tibial fractures.


Several elective cases of mal-unions and non-unions as well as complications were operated during our stay. Due to a wide array of instruments and implants, various possibilities of problem-solving and internal fixation could be demonstrated.

Equipment in OT was very good compared to PNG standards. An almost new and perfectly working C-arm was available, enabling a much higher standard of safety, especially in nailing procedures on the femur. Working with intraoperative imaging has to be instructed in regard to radiation protection, sterility and technique.
The main problem we were facing was the inability to get patients – even with relatively urgent indications – into OT. The cancellation rate as well as the resulting waiting time was very high, even due to inacceptable reasons. Due to this limited OT capacity, it seems to be very hard for the surgical team to provide a sufficient basic trauma care. Admitted patients often wait for days and weeks, until initial operative treatment is carried out.
Conclusions:
The introduction of the SIGN system can be considered successful, even though the number of treated patients could have been much higher. The future will tell if a sufficient number of SIGN cases will be reported in order to sustain the program.
Various other cases were operated on during our stay, but the overall efficiency of our visitation was restricted due to limited time in OT.
Several suggestions to optimize workflows in clinics and OT were made. Full use of available resources, guidelines to standardize trauma care (including use of antibiotics) would lead to a more efficient trauma service, shorter length of stay in hospital, less complications and better functional results. Angau Hospital in Lae, serving a very large population and dealing with a heavy burden of trauma, would be a very important place for future educational projects within PIOA. A future visit for further evaluation and continuing education will be planned.